Tales from Coronavee-rooss Italy, mamma mia!
-
-
@Gąska said in Tales from Coronavee-rooss Italy, mamma mia!:
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
Sometimes kids burn alive because they couldn't get out of their seatbelt quickly enough.
Do they? Can't find any source. And I'm not just being contrarian; it seems like one of those things that everyone assumes must necessarily happen from time to time because it sounds logical, but there seem to be no actual examples of it.
People unable to get out of the seatbelts tend to be too incapacitated to move anyway. usually because the fire follows a fierce crash.
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@topspin said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
I have to ask whether these are hospitalizations from COVID, or with COVID.
It's funny that this always gets mentioned for Covid cases, but then we're talking about VAERS data which doesn't even claim to make this distinction, as anybody can report anything that happened post hoc, so is massively overreported with background signal.
Actually, only medical personnel can report to VAERS. So over-counting is unlikely.
And I assume that the report contents are more useful than what we have in Finland.
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@topspin said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
I have to ask whether these are hospitalizations from COVID, or with COVID.
It's funny that this always gets mentioned for Covid cases, but then we're talking about VAERS data which doesn't even claim to make this distinction, as anybody can report anything that happened post hoc, so is massively overreported with background signal.
Actually, only medical personnel can report to VAERS. So over-counting is unlikely.
And I assume that the report contents are more useful than what we have in Finland.Underreporting is estimated to be between 10 and 100 times. For all vaccines and drugs, not only for covid stuff.
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
only medical personnel can report to VAERS. So over-counting is unlikely.
The same medical personnel you don't trust to report if something is because of or with covid you now trust to distinguish between because of the vaccine or happened after the vaccine?
And "parents and patients" are probably no better at making that distinction. They don't have to, either, they're just supposed to report and not diagnose the cause.
-
@boomzilla said in Tales from Coronavee-rooss Italy, mamma mia!:
Well, they were lying because they think it's better for the public. That's the definition.
Yeah, but I think not all the lying was because they think it was better for the public. Call me cynical, but I think a not-insignificant part of the lying was because they think it's better for the liars. Undeniably, the panic has made certain elite politicians, doctors and media more powerful.
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
Obviously. We can compare the frequency of those when we include other non-lethal effects of infections, too. But as you cited infection fatality ratios only, let's compare equal risks, shall we?
Fine. I've got numbers from Finland for 2020. Those good?
Deaths in the age group 0-19 while Sars-CoV2 -positive: 0.
Deaths in age group 20-24 for same: 1.I don't think with 558 total deaths the statistic is anywhere as solid as with 800k+. It doesn't help you calculate the numerical risk of not surviving the vaccine anyway.
I hear some diabetic teens died
this yearin 2021. But no statistics yet. The official page for the statistics agency says that the statistics for 2021 will not be published until end of 2022.
The reason for that is explained in the first paragraph.
-
@topspin said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
only medical personnel can report to VAERS. So over-counting is unlikely.
The same medical personnel you don't trust to report if something is because of or with covid you now trust to distinguish between because of the vaccine or happened after the vaccine?
And "parents and patients" are probably no better at making that distinction. They don't have to, either, they're just supposed to report and not diagnose the cause.
I think the point is that you're gonna have fewer spurious reports if you actually need to be a medical worker to report, as opposed to what would happen if reporting was open to general public.
-
@topspin said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@topspin said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
I have to ask whether these are hospitalizations from COVID, or with COVID.
It's funny that this always gets mentioned for Covid cases, but then we're talking about VAERS data which doesn't even claim to make this distinction, as anybody can report anything that happened post hoc, so is massively overreported with background signal.
Actually, only medical personnel can report to VAERS. So over-counting is unlikely.
And I assume that the report contents are more useful than what we have in Finland.Huh. Didn't know that.
Still, the information available doesn't really sell the vaccine. Especially for my children. You do you.
-
@GOG said in Tales from Coronavee-rooss Italy, mamma mia!:
@topspin said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
only medical personnel can report to VAERS. So over-counting is unlikely.
The same medical personnel you don't trust to report if something is because of or with covid you now trust to distinguish between because of the vaccine or happened after the vaccine?
And "parents and patients" are probably no better at making that distinction. They don't have to, either, they're just supposed to report and not diagnose the cause.
I think the point is that you're gonna have fewer spurious reports if you actually need to be a medical worker to report, as opposed to what would happen if reporting was open to general public.
That's true, but since it's the covid hospitalizations where the medical workers report and the VAERS data where the general public reports, it's counter-factual and irrelevant.
-
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
Obviously. We can compare the frequency of those when we include other non-lethal effects of infections, too. But as you cited infection fatality ratios only, let's compare equal risks, shall we?
Fine. I've got numbers from Finland for 2020. Those good?
Deaths in the age group 0-19 while Sars-CoV2 -positive: 0.
Deaths in age group 20-24 for same: 1.I don't think with 558 total deaths the statistic is anywhere as solid as with 800k+. It doesn't help you calculate the numerical risk of not surviving the vaccine anyway.
Point was rather that both numbers are too small to properly estimate in Finland. And rather moot since it looks like we all get COVID before end of the year.
I hear some diabetic teens died
this yearin 2021. But no statistics yet. The official page for the statistics agency says that the statistics for 2021 will not be published until end of 2022.The reason for that is explained in the first paragraph.
Yes. And it makes me amazed at the slow movements of the bureaucracy. You'd think with a global pandemic underway they could calculate those stats with a brisker pace.
-
@MrL said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@topspin said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
I have to ask whether these are hospitalizations from COVID, or with COVID.
It's funny that this always gets mentioned for Covid cases, but then we're talking about VAERS data which doesn't even claim to make this distinction, as anybody can report anything that happened post hoc, so is massively overreported with background signal.
Actually, only medical personnel can report to VAERS. So over-counting is unlikely.
And I assume that the report contents are more useful than what we have in Finland.Underreporting is estimated to be between 10 and 100 times. For all vaccines and drugs, not only for covid stuff.
Sounds reasonable.

I know I dutifully reported my side effects after my COVID vaccination (the first, and so far only, vaccination I've gotten since VAERS existed; I wish it had existed ~30 years ago when I got my last tetanus booster; that was nasty), even though after about 2-3 days the report was that there were no symptoms to report. I still get occasional text messages reminding me to report, although after about a month I started ignoring them.
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@topspin said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
I have to ask whether these are hospitalizations from COVID, or with COVID.
It's funny that this always gets mentioned for Covid cases, but then we're talking about VAERS data which doesn't even claim to make this distinction, as anybody can report anything that happened post hoc, so is massively overreported with background signal.
Actually, only medical personnel can report to VAERS. So over-counting is unlikely.
And I assume that the report contents are more useful than what we have in Finland.I got sent a link to sign up and report stuff after my rona shot. My guess is that they don't normally do that for approved vaccines, but they were all still under emergency (or whatever) approval at the time.
-
@MrL said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@topspin said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
I have to ask whether these are hospitalizations from COVID, or with COVID.
It's funny that this always gets mentioned for Covid cases, but then we're talking about VAERS data which doesn't even claim to make this distinction, as anybody can report anything that happened post hoc, so is massively overreported with background signal.
Actually, only medical personnel can report to VAERS. So over-counting is unlikely.
And I assume that the report contents are more useful than what we have in Finland.Underreporting is estimated to be between 10 and 100 times. For all vaccines and drugs, not only for covid stuff.
Typically, yes. But the high volume of reports is now countered with the claim that people are overreporting due to COVID politics.
Why all these systems can't separate the reports by reporter type (pro / layman) upon receipt is beyond me.
-
@HardwareGeek said in Tales from Coronavee-rooss Italy, mamma mia!:
@boomzilla said in Tales from Coronavee-rooss Italy, mamma mia!:
Well, they were lying because they think it's better for the public. That's the definition.
Yeah, but I think not all the lying was because they think it was better for the public. Call me cynical, but I think a not-insignificant part of the lying was because they think it's better for the liars. Undeniably, the panic has made certain elite politicians, doctors and media more powerful.
Yeah, hence my example of the lab leak thingy. But I think most of the masking and most of the vaccine campaigns qualify.
-
@boomzilla said in Tales from Coronavee-rooss Italy, mamma mia!:
I got sent a link to sign up and report stuff after my rona shot. My guess is that they don't normally do that for approved vaccines, but they were all still under emergency (or whatever) approval at the time.
I was given that at the time of the vaccination. I don't know whether it's normal for other vaccinations, since I haven't had any other vaccinations recently, or just because of the not-fully-approved status of this vaccine. In any case, I had to wait on-site ~15 minutes, in case there was any immediate, severe side effect (like anaphylaxis), and I signed up on my phone and made my first report (dur, I just got stabbed in the arm with a metal needle; it's slightly sore) during that 15 minute wait.
-
@Gąska said in Tales from Coronavee-rooss Italy, mamma mia!:
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
Sometimes kids burn alive because they couldn't get out of their seatbelt quickly enough.
Do they? Can't find any source. And I'm not just being contrarian; it seems like one of those things that everyone assumes must necessarily happen from time to time because it sounds logical, but there seem to be no actual examples of it.
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@MrL said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@topspin said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
I have to ask whether these are hospitalizations from COVID, or with COVID.
It's funny that this always gets mentioned for Covid cases, but then we're talking about VAERS data which doesn't even claim to make this distinction, as anybody can report anything that happened post hoc, so is massively overreported with background signal.
Actually, only medical personnel can report to VAERS. So over-counting is unlikely.
And I assume that the report contents are more useful than what we have in Finland.Underreporting is estimated to be between 10 and 100 times. For all vaccines and drugs, not only for covid stuff.
Typically, yes. But the high volume of reports is now countered with the claim that people are overreporting due to COVID politics.
Why all these systems can't separate the reports by reporter type (pro / layman) upon receipt is beyond me.On the other hand we have all those reports (or stories) from people claiming that doctors refused to report their side effects

-
@HardwareGeek said in Tales from Coronavee-rooss Italy, mamma mia!:
@boomzilla said in Tales from Coronavee-rooss Italy, mamma mia!:
I got sent a link to sign up and report stuff after my rona shot. My guess is that they don't normally do that for approved vaccines, but they were all still under emergency (or whatever) approval at the time.
I was given that at the time of the vaccination. I don't know whether it's normal for other vaccinations, since I haven't had any other vaccinations recently, or just because of the not-fully-approved status of this vaccine. In any case, I had to wait on-site ~15 minutes, in case there was any immediate, severe side effect (like anaphylaxis), and I signed up on my phone and made my first report (dur, I just got stabbed in the arm with a metal needle; it's slightly sore) during that 15 minute wait.
Yeah, I did the sitting around thing, too. I think I got the link in a follow up email, but then it could have been in the appointment emails. I don't recall. It may not surprise you that I didn't sign up.
-
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
@Gąska said in Tales from Coronavee-rooss Italy, mamma mia!:
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
Sometimes kids burn alive because they couldn't get out of their seatbelt quickly enough.
Do they? Can't find any source. And I'm not just being contrarian; it seems like one of those things that everyone assumes must necessarily happen from time to time because it sounds logical, but there seem to be no actual examples of it.
Note that the last one was in 1993. And a lot of the entries are very questionable. Also I couldn't confirm any of the ones I googled, but that might be just a failure of the internet in keeping track of pre-internet stuff.
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
I have to ask whether these are hospitalizations from COVID, or with COVID. Because the U.S. officials recently admitted their statistics mixing the two.
My understanding is that these numbers are always "with COVID" rather than "from COVID", because it's the only clean statistic you can get; "from COVID" always requires someone to do a judgement call, which will introduce bias. For "with COVID", you at least know what you're measuring.
Imagine some guy's adimtted to hospital because of a heart attack. The COVID test at hospital is positive. Would he have had the heart attack if he hadn't had COVID? Who decides that, and how?
-
@ixvedeusi said in Tales from Coronavee-rooss Italy, mamma mia!:
My understanding is that these numbers are always "with COVID" rather than "from COVID", because it's the only clean statistic you can get; "from COVID" always requires someone to do a judgement call, which will introduce bias. For "with COVID", you at least know what you're measuring.
Imagine some guy's adimtted to hospital because of a heart attack. The COVID test at hospital is positive. Would he have had the heart attack if he hadn't had COVID? Who decides that, and how?There's been some analyses of that (I saw a summary ages ago) and the difference tends to be a bit moot, with the death rate “from COVID” being very close to the death rate “with COVID”. But the former is slow to determine (potentially requiring a coroner and inquest) whereas the latter is pretty quick, mostly being covered by medical records.
-
@dkf said in Tales from Coronavee-rooss Italy, mamma mia!:
potentially requiring a coroner and inquest
And when it's about hospitalizations rather than deaths you don't really have that option.
-
@ixvedeusi I get the point. But with no screening whatsoever, we get traffic accident victims counted as covid hospitalizations. It is possible to calculate a somewhat better estimate from that raw number, yes. But it's not easy, since you have to take into account all kinds of real-life phenomena. Like hospitals hitting some kind of capacity limit on staff/devices/facilities, and with COVID patient ratio decreasing as a result in an unexpected manner (or increasing; life is funny). And then people will have to trust whomever makes that calculation.
I think separating the cases on a transparent criteria would be a better idea. Like e.g. on whether there were breathing issues, or airway-related treatments needed, would give a fairer assessment. Maybe include a couple of the most common other types of symptoms of COVID that people seek help for, but only if they got a positive antigen test.
-
@dkf
I remember very recent news articles on CDC admitting that there was a large difference. It was discussed in the Garage threads.Nevermind. It was hospitalizations, and you were talking deaths.
-
@acrow Ah. Here we go:
 Healthline: Medical information and health advice you can trust.
Healthline: Medical information and health advice you can trust.

We're committed to being your source for expert health guidance. Come to us in your pursuit of wellness.
In New York, 57 percent of coronavirus-positive patients were admitted “for COVID,” while the rest were admitted “with COVID.”
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
It is possible to calculate a somewhat better estimate from that raw number, yes. But it's not easy
Agreed. I suppose you'll have to subtract some kind of "base hospitalization rate", which of course introduces any error you have on that rate into your results. Still, for doing science I do believe it's the only valid approach. Do anything else and you've pre-filtered your data with forgone conclusions and will end up confirming your expectations.
But I agree it's not at all what a layman would expect the number to represent, and so it's misleading when used in public communications. For that use I'd think that breaking out the "clearly due to COVID" numbers (or applying the above mentioned base rate correction, or at least always showing the base rate alongside) would probably be more honest.
-
@dkf said in Tales from Coronavee-rooss Italy, mamma mia!:
@ixvedeusi said in Tales from Coronavee-rooss Italy, mamma mia!:
My understanding is that these numbers are always "with COVID" rather than "from COVID", because it's the only clean statistic you can get; "from COVID" always requires someone to do a judgement call, which will introduce bias. For "with COVID", you at least know what you're measuring.
Imagine some guy's adimtted to hospital because of a heart attack. The COVID test at hospital is positive. Would he have had the heart attack if he hadn't had COVID? Who decides that, and how?There's been some analyses of that (I saw a summary ages ago) and the difference tends to be a bit moot, with the death rate “from COVID” being very close to the death rate “with COVID”. But the former is slow to determine (potentially requiring a coroner and inquest) whereas the latter is pretty quick, mostly being covered by medical records.
I read a news article earlier this week which mentioned that because infection rates are going up fast and admittence rates are trending downwards, the 'with but not due to COVID' admittance rate was becoming relevant. This does not matter a lot to hospitals because they need to apply COVID quarantine anyway, but it is important politically for capacity planning, lockdown policy, etc.
In related items, numbers are looking awesome here (except for the positive test ones).
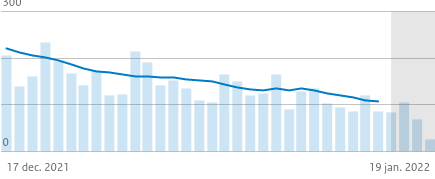
(source)That's general hospitalizations. Including with-but-not-due-to.
If this trend holds we'll be down to zero by the end of next month. We might actually have a King's Day this year.
-
@ixvedeusi said in Tales from Coronavee-rooss Italy, mamma mia!:
But I agree it's not at all what a layman would expect the number to represent, and so it's misleading when used in public communications.
Not only that. Civic leaders are also laymen. And it is them who have to make the final call. To wield the power and bear the responsibility, if you will.
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
and bear the responsibility
Very strong

-
@MrL said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
and bear the responsibility
Very strong
In theory anyway.
Ehh... If you make a big enough screw-up, the consequences will come around. One way or another. I doubt our current PM will have very lucrative career options open to her, once the current term is over.
-
@PleegWat said in Tales from Coronavee-rooss Italy, mamma mia!:
I read a news article earlier this week which mentioned that because infection rates are going up fast and admittence rates are trending downwards, the 'with but not due to COVID' admittance rate was becoming relevant. This does not matter a lot to hospitals because they need to apply COVID quarantine anyway, but it is important politically for capacity planning, lockdown policy, etc.
You can cross reference it against excess load figures; if COVID is just something that isn't causing much hospitalization (“with” dominant) then the amount of loading on hospitals should be close to that in a normal pre-pandemic year, as there probably should be about the same number of heart attacks, strokes, cancers, broken legs, etc. as usual. It won't be a perfect measure (because the presence of COVID has changed people's behaviours somewhat, especially among people more likely to suffer from serious consequences of any infection) but it does give you a way to figure out if you've at least got close to understanding what's going on.
Pandemics are big signals. It should be possible, even easy, to spot the outcomes using multiple methods.
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@MrL said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
and bear the responsibility
Very strong
In theory anyway.
Ehh... If you make a big enough screw-up, the consequences will come around. One way or another. I doubt our current PM will have very lucrative career options open to her, once the current term is over.I've seen screw ups of monumental scale with no repercussions whatsoever and the guilty marrily continuing their successful careers. Sometimes there are consequences though, true.
But since we are talking about covid, my prediction: literally noone (from covidian camp) will bear any responsibility for their actions during the pandemic.
I'll narrow down this to Poland, since I don't know enough about how fucked up other countries are.
-
@MrL said in Tales from Coronavee-rooss Italy, mamma mia!:
I don't know enough about how fucked up other countries are.
 : More fucked than even
: More fucked than even can manage.
-
@dkf Speaking of which. I pondered some more on the importance, or lack thereof, of knowing the exact infection-reducing quality of the vaccine. There is a good reason for figuring it out as exactly as possible: human behavior.
Relatively massive events like music festivals were held in e.g. U.K.. And all event-goers had to have a vaccine pass. I'm not sure if a negative test result was also accepted. But the festivals turned out to be such super-spread events that briefly there were more vaccinated COVID hospitalizations than un-vaccinated.
Now, if the vaccine could reduce infections by 94% (hypothetical, but I think some civic leaders read the Pfizer press release of their original study this way), then allowing that kinda festivals to be arranged as long as everyone is vaccinated would be probably OK. Maybe?
Whereas if the reduction in infection is in the order of 50%, then allowing a festival is obviously not safe to do.
-
@dkf said in Tales from Coronavee-rooss Italy, mamma mia!:
@MrL said in Tales from Coronavee-rooss Italy, mamma mia!:
I don't know enough about how fucked up other countries are.
: More fucked than even  : More fucked up than that. We've got nurses resigning in massive quantities. No, not because of the vaccine mandate; they can keep their jobs in spite of that due to lack of anyone to replace them. We've got nurses resigning due to low pay and excessive workload. And the workload was excessive before the pandemic. Chronically understaffed hospitals.
: More fucked up than that. We've got nurses resigning in massive quantities. No, not because of the vaccine mandate; they can keep their jobs in spite of that due to lack of anyone to replace them. We've got nurses resigning due to low pay and excessive workload. And the workload was excessive before the pandemic. Chronically understaffed hospitals.
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
I pondered some more on the importance, or lack thereof, of knowing the exact infection-reducing quality of the vaccine. There is a good reason for figuring it out as exactly as possible: human behavior.
It seems to be complicated, with factors like which variant, which vaccine (or mix of vaccines) delivered when, what previous infections, what sort of venue, what sort of event, etc.
-
@dkf said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
I pondered some more on the importance, or lack thereof, of knowing the exact infection-reducing quality of the vaccine. There is a good reason for figuring it out as exactly as possible: human behavior.
It seems to be complicated, with factors like which variant, which vaccine (or mix of vaccines) delivered when, what previous infections, what sort of venue, what sort of event, etc.
Figuring it out is hard, yes. But having some kind of measured figure would have made a large difference by now. Because, say, 25%, 50% and 90% reductions will have a huge difference in what kinds of events you can safely Green Pass.
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
Figuring it out is hard, yes. But having some kind of measured figure would have made a large difference by now. Because, say, 25%, 50% and 90% reductions will have a huge difference in what kinds of events you can safely Green Pass.
The problem is that first factor I mentioned: which variant. Basic mitigations that made events safe with alpha are insufficient with omicron due to the latter's vastly higher infectiousness.
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
Relatively massive events like music festivals were held in e.g. U.K.. And all event-goers had to have a vaccine pass. I'm not sure if a negative test result was also accepted.
In England at least negative tests were acceptable as was having tested positive within the last 180 days (but not the last 10). Both of these are still true for the COVID pass in England.
The earlier pilot events (like Download in June) took place before anyone under 40 was likely to have been fully vaccinated and testing negative was the only requirement.
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@dkf Speaking of which. I pondered some more on the importance, or lack thereof, of knowing the exact infection-reducing quality of the vaccine. There is a good reason for figuring it out as exactly as possible: human behavior.
Relatively massive events like music festivals were held in e.g. U.K.. And all event-goers had to have a vaccine pass. I'm not sure if a negative test result was also accepted. But the festivals turned out to be such super-spread events that briefly there were more vaccinated COVID hospitalizations than un-vaccinated.
Now, if the vaccine could reduce infections by 94% (hypothetical, but I think some civic leaders read the Pfizer press release of their original study this way), then allowing that kinda festivals to be arranged as long as everyone is vaccinated would be probably OK. Maybe?
Whereas if the reduction in infection is in the order of 50%, then allowing a festival is obviously not safe to do.That is true, but it's a political problem and not a vaccine study / admission problem. Especially not if you don't believe the transmission reduction was always 0% and the scientists just lied, politicians making wrong claims notwithstanding.
We've seen this exact effect here in Germany too, where the restrictions for some of the less fundamental "leisure" activities last year went from what we called 3G (for recovered, tested, or vaccinated) to 2G (recovered or vaccinated) when it was still assumed to have a relevant effect on transmissibility. It became clear with delta that this effect is much lower than hoped for, so they made the sensible change to (recovered or vaccinated and tested), which worked out pretty well. This was an evidence-based decision. But then they started the booster campaign and politically decided that the "tested" requirement could be dropped for people with the booster shot. This is obviously contrary to what we know, as admitted by their own previous rule changes, and counter-productive.
But it shows that waiting to admit the vaccine until all possible long-term effects are known, besides being futile for a changing virus, wouldn't prevent stupid political decisions made when exactly these things are known.
-
@dkf said in Tales from Coronavee-rooss Italy, mamma mia!:
@MrL said in Tales from Coronavee-rooss Italy, mamma mia!:
I don't know enough about how fucked up other countries are.
: More fucked than even
-
@Applied-Mediocrity said in Tales from Coronavee-rooss Italy, mamma mia!:
@dkf said in Tales from Coronavee-rooss Italy, mamma mia!:
@MrL said in Tales from Coronavee-rooss Italy, mamma mia!:
I don't know enough about how fucked up other countries are.
: More fucked than even It's @Tsaukpaetra versus BoJo the sneering contemptuous crooked bullying lying stupid mendacious philandering lazy
 . (I believe there's evidence for all parts of that description except the bit that actively involves wearing white makeup and outsize shoes.)
. (I believe there's evidence for all parts of that description except the bit that actively involves wearing white makeup and outsize shoes.)You might conclude that I'm not very impressed with a certain politician.
-
@dkf said in Tales from Coronavee-rooss Italy, mamma mia!:
You might conclude that I'm not very impressed with a certain politician.
Whenever you get that feeling, try to remember that every candidate for the elections is put forth by cadre of politicians who all think he's a good idea. After knowing him for far longer than the voters do.
...The one that got elected doesn't seem so bad now, does he?
-
@dkf said in Tales from Coronavee-rooss Italy, mamma mia!:
Pandemics are big signals. It should be possible, even easy, to spot the outcomes using multiple methods.
Yes. It's just that we're mostly not doing that. And we've done it wrong enough that now it's difficult to trust that anyone is getting better at it. Just as an example, public discourse has almost always been focused on total deaths with COVID, and these numbers were almost always without any context. For sure COVID killed a lot of people who probably wouldn't have died then, but we haven't been able to take a reasonable look at the actual effects, and we also mostly haven't been able to consider the consequences of our panic.
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
The one that got elected doesn't seem so bad now, does he?
I don't like his party either, but then I've not voted for them for a long time. (They used to have a very good local candidate, one of the old type of politician who was conspicuous in doing his best for all his electorate, and was wildly popular as a result. There's a lesson in this for the current crop, if only they could bring themselves to listen to it.)
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
Whenever you get that feeling, try to remember that every candidate for the elections is put forth by cadre of
politicianspermanently rooted port-sipping career functionariesAs outlined by the excellent educational documentaries "Yes, Minister" and "Yes, Prime Minister".
-
@ixvedeusi said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
I have to ask whether these are hospitalizations from COVID, or with COVID. Because the U.S. officials recently admitted their statistics mixing the two.
My understanding is that these numbers are always "with COVID" rather than "from COVID", because it's the only clean statistic you can get; "from COVID" always requires someone to do a judgement call, which will introduce bias. For "with COVID", you at least know what you're measuring.
An objective but useless measure is worse than a subjective but useful measure. Compare to memory use by processes. In Windows, the Task Manager is lying by selectively omitting certain allocations, to give you a more or less real picture how much memory a process uses. In Linux, you have resident memory which is 100% accurate but much less than total memory used, and shared memory which is also 100% accurate but much more than total memory used - leaving you with no idea how much memory a process actually uses.
-
@boomzilla said in Tales from Coronavee-rooss Italy, mamma mia!:
For sure COVID killed a lot of people who probably wouldn't have died then, but ...
... many of whom were so ill they probably would have died soon from almost any cause.
-
@HardwareGeek said in Tales from Coronavee-rooss Italy, mamma mia!:
@boomzilla said in Tales from Coronavee-rooss Italy, mamma mia!:
For sure COVID killed a lot of people who probably wouldn't have died then, but ...
... many of whom were so ill they probably would have died soon from almost any cause.
As one of Polish experts explained (I think his name is Kuna), and I'm paraphrasing heavily here:
"Many diseases can be a compounding factor of death. Let's take an example. Flu kills a lot of people every year. When a patient is admitted to hospital with flu, and he has a history of serious heart problems - flu puts a strain on his system, his existing conditions worsen. Finally he dies of heart attack. In that case we put 'heart disease' on death certificate - it's the heart condition that killed him, flu just sped up the process. Covid is the only disease when we do the opposite, doesn't matter what killed the patient, covid is on the certificate. Covid can kill on its own, with lungs inflamation, but that's just a fraction of reported covid deaths."