Tales from Coronavee-rooss Italy, mamma mia!
-
@boomzilla said in Tales from Coronavee-rooss Italy, mamma mia!:
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
@boomzilla said in Tales from Coronavee-rooss Italy, mamma mia!:
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
@Gąska said in Tales from Coronavee-rooss Italy, mamma mia!:
@dkf the problem with hypothetical avoidable deaths is that there are infinitely many of them,
With a finite number of people alive?
and you cannot even estimate them most of the time. For example, if we didn't fast-track the vaccines, less people would be skeptical of them - and by today we'd end up with many more vaccinated.
No. By today we'd have precisely zero vaccinated outsides clinical trials, because the approval would be expected around 2025.
Most of the time savings in the fast-track process (aside from simply treating it as prio 1 in the bureaucracy of course) was from interleaving the trial phases, which is usually not done because you don't want to expose a large number of volunteers to something you haven't checked is safe. That interleaving has zero influence on the validity of the results.
Except we'd could have had more data on the medium term effects, i.e., the waning efficacy.
What could possibly have been the consequence of having this data?
a) go ahead and use the vaccine anyway
b) decide it's no good, wait without any vaccinations until we have developed something better and let it go through the multi-year approval process againAny other possibilities?
Edit:
 by
by 
Also there could have been more focus on therapeutics. Aside from a governor or two here, it's been all about the vaccines. I get the impression that they believed that focusing on anything but the vaccines would make people care less about them. Instead they went crazy about the vaccines and freaked people out even more.
There's been a lot of noble lying on public health. If nothing else these people could have kept some credibility for the future.
Oh, also, the continued focus on vaccine passport type of stuff. If the vaccines prevented spread then they could kinda make some logical sense, even if you don't believe they pass the smell test otherwise, but there's really no justification for it other than to coerce people to get vaccinated.
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@topspin said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
Also, e.g. Pfizer's 94% efficiency number was based on 1 vs 18 cases of COVID-19 (the syndrome, not the virus), which is not statistically rigorous.
What is the statistically rigorous number then?
If we're expecting two meaningful digits in the results, then I want to see at least two digits in both test groups.
You didn't answer the question, I assume you mean "90%+".
Just use the confidence intervals then if you want to be accurate. Studies give those when they present data.@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@topspin said in Tales from Coronavee-rooss Italy, mamma mia!:
@MrL said in Tales from Coronavee-rooss Italy, mamma mia!:
@topspin said in Tales from Coronavee-rooss Italy, mamma mia!:
Risk for younger people with no co-morbidities approaches statistical zero the younger you get. This was known rather early.
And risk for everyone except those specifically excluded for the vaccine "approaches statistical zero".
It doesn't. Unless you think that 1/1000 for mild side effects and 1/2500 for serious ones, including death, is approaching zero.
That's from VAERS, statistics from some other systems look even worse.
I'm using the same "definition" as the one used in the quote.
So you're claiming that side-effects from the vaccine get less frequent the younger the recipient? Fascinating. I'd like to see your data for this.
I didn't say anything about age, only about the comparison to basically zero.
-
@topspin Mathematically approaching zero has a specific meaning, when going to a certain direction in the inputs.
In this case it means that bad cases of covid for young people get increasingly rare, the younger we're talking about. Never zero. But so rare that it's impossible to give a meaningful number statistically, when we get young enough.
-
@topspin I never said there were "basically zero" cases in the young. Only that they "approach zero" statistically.
-
@boomzilla said in Tales from Coronavee-rooss Italy, mamma mia!:
they went crazy about the vaccines and freaked people out even more
Even worse, here in the States, the protocol was - perhaps, still is - the following:
- "go back home and stay there until you have trouble breathing," by which time your blood O2 is not much above danger zone, if you're lucky - oh, and of course, no significant medication or other treatment is given when you present initially
- when you finally do go back in, the hospital puts you on a vent, which is by itself known to be very difficult to stop needing (except when you die, of course)
- the hospital also puts you on remdesivir, which is by itself known to cause potentially severe organ damage
Of course, in the world of corporate medicine, no one deviates from the protocol without a fight. Also, no one asks how many of the "COVID" deaths involved a vent, remdesivir, or being told to stay home until you have trouble breathing.
-
@lolwhat said in Tales from Coronavee-rooss Italy, mamma mia!:
Also, no one asks how many of the "COVID" deaths involved a vent or remdesivir.
I know two people who took Remdesivir in the hospital and started feeling better almost immediately and soon after went home. I've heard the jokes about Remdesivir but I'm not sure they're well grounded, statistically or medically. Of course if you wait long enough on a patient who's going to die, there's probably no treatment that will save them.
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
Any other possibilities?
Limit use to places where it'll do the most good anyway? Like, say, old people?
That's "a) go ahead and use the vaccine anyway". But how is limiting the population to vaccinate related to data on waning efficacy?
Because then you can actually time your vaccinations to the start of the flu season, when most of the infections and deaths happen?
I don't understand. If you have data on waning efficacy, you can limit vaccine use to old people and time it to the start of the flu season, which you cannot do if you don't have this data?
As it happened, governments started vaccinating middle-aged and younger people in the middle of the summer. VAERS data is still being processed, but the side-effects weren't exactly non-existent. For little actual benefit.
What's the numeric risk of not surviving the vaccine for the 0-19 group?
Less pressure on the virus to start evading vaccines that way.
And more opportunities for spontaneous mutations, cf. Omicron.
You assume that the vaccines limit infection. For which there is no evidence.
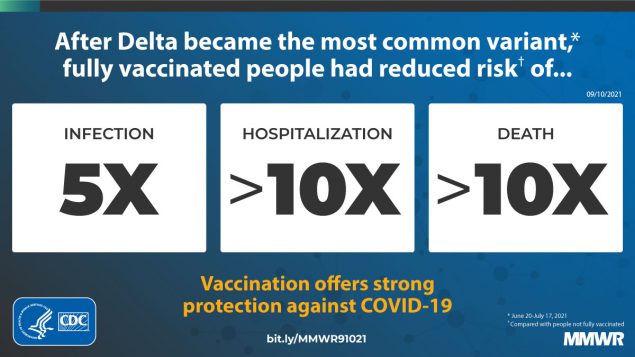
That infection rate figure is rather hopeful. It's not based on solid evidence. there's been no population screening. The hospitalization and death rate I'll buy, sure. But if that infection rate reduction were real, we'd be seeing large differences between nations based on vaccine coverage.
Why would you believe your infection fatality rates from the same source are based on solid evidence if the infection rates they are based on are not?
Besides, they'd only have to reduce transmission, as a mutation that doesn't get transmitted might as well not exist.
If you don't believe they reduce either, what do you think casues this pressure on the virus to start evading vaccines?Finally a good question. It's a double-edged sword:
- If the vaccine reduces infections enough to be relevant on population level, but does not enough to potentially eradicate the virus in short order, then the virus will mutate to evade it.
You said there is "no evidence" that "vaccines limit infection". How would vaccinating fewer people lead to "less pressure on the virus to start evading vaccines that way"?
- If the vaccine doesn't reduce infections, then vaccinating those with little or no chance of bad outcomes from the virus makes no sense, as there are always some side effects even if we were jabbing plain saline.
If death was the only possible bad outcome and the seemingly low numbers for the 20-69 group weren't enough to still overfill hospitals with what counts as "mild" cases, then yes.
-
@boomzilla said in Tales from Coronavee-rooss Italy, mamma mia!:
I know two people who took Remdesivir in the hospital and started feeling better almost immediately and soon after went home.
I've heard of several that went the other way. Too bad I don't know of any collection of such data.
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@topspin Mathematically approaching zero has a specific meaning, when going to a certain direction in the inputs.
In this case it means that bad cases of covid for young people get increasingly rare, the younger we're talking about. Never zero. But so rare that it's impossible to give a meaningful number statistically, when we get young enough.And exclude the too-young so as not to spoil the mathematical beauty.
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
Only that they "approach zero" statistically.
That's not a helpful comment. It's much more helpful to compare rates, which are essentially (approximate) ratios. Those can be sensibly compared. For example, we can say that the rate of death due to the virus in unvaccinated primary school age children is lower than the rate of death due to the virus in unvaccinated senior citizens, and this appears to be the case in all countries in the world. We can also compare when we allow more variables to change at once, but then it's enormously harder to pull the sense out of what's being said. Comparing rates between countries is trickier, because there's often many public policy differences between them, and that affects all sorts of aspects of social behaviour.
One thing that can be said is that the rate of serious side effects from the majority of vaccines in deployment appear to be multiple orders of magnitude lower than the population average rate of serious outcomes from coronaviral infections among the unvaccinated. (In both of these cases, we can take “serious” as meaning either that hospitalization is required or that the person becomes effectively disabled for an extended period.) The exact rates might not be known, but when there's several orders of magnitude of difference we can have a reasonably high degree of confidence in the sort order between the two; for the rate of either to change by as much as an order of magnitude would be highly surprising.
-
@boomzilla said in Tales from Coronavee-rooss Italy, mamma mia!:
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
@boomzilla said in Tales from Coronavee-rooss Italy, mamma mia!:
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
@Gąska said in Tales from Coronavee-rooss Italy, mamma mia!:
@dkf the problem with hypothetical avoidable deaths is that there are infinitely many of them,
With a finite number of people alive?
and you cannot even estimate them most of the time. For example, if we didn't fast-track the vaccines, less people would be skeptical of them - and by today we'd end up with many more vaccinated.
No. By today we'd have precisely zero vaccinated outsides clinical trials, because the approval would be expected around 2025.
Most of the time savings in the fast-track process (aside from simply treating it as prio 1 in the bureaucracy of course) was from interleaving the trial phases, which is usually not done because you don't want to expose a large number of volunteers to something you haven't checked is safe. That interleaving has zero influence on the validity of the results.
Except we'd could have had more data on the medium term effects, i.e., the waning efficacy.
What could possibly have been the consequence of having this data?
a) go ahead and use the vaccine anyway
b) decide it's no good, wait without any vaccinations until we have developed something better and let it go through the multi-year approval process againAny other possibilities?
Edit:
by Also there could have been more focus on therapeutics. Aside from a governor or two here, it's been all about the vaccines.
What do you mean by "focus"? Do you see a lack of government funding for therapeutic research or would you just want politicians to talk about it more?
-
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
How would vaccinating fewer people lead to "less pressure on the virus to start evading vaccines that way"?
Ugh, evolution doesn't work that way. The formation of new variants is a random process — every time the virus reproduces you roll the dice to see if you get a new variant, and occasionally those new variants are better adapted to their environment — but if we can reduce the rate at which the virus reproduces then we increase the expected time to the appearance of new variants that are better able to avoid vaccine-induced immunity. The lower the overall population infection rate, the less likely you are to roll snake eyes somewhere and have a new pile of shit to deal with.
-
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
What's the numeric risk of not surviving the vaccine for the 0-19 group?
Death is not the only issue. Some of the other side-effects are rather bad too. E.g.:
Why would you believe your infection fatality rates from the same source are based on solid evidence if the infection rates they are based on are not?
Because the count of deaths has a known source material (death certificates) available to the reporting entity (U.S. CDC), which reports all of them. And it's plausible that they can find out the vaccination status of each dead person. So it's technically plausible to count this number, even though the died from vs died with debate puts its exactness to some doubt.
Whereas infections are based on people's reporting only. There's no population screening, or any mechanism that would give a rate without human bias. And people who got the vaccination are biased to believe that their couch is not COVID, since they are vaccinated.
You said there is "no evidence" that "vaccines limit infection". How would vaccinating fewer people lead to "less pressure on the virus to start evading vaccines that way"?
"No evidence" does not mean that it can't happen. It just means we can't know whether it happens or not. And if it limited infection, then it soon won't, so the point is moot.
-
@dkf said in Tales from Coronavee-rooss Italy, mamma mia!:
One thing that can be said is that the rate of serious side effects from the majority of vaccines in deployment appear to be multiple orders of magnitude lower than the population average rate of serious outcomes from coronaviral infections among the unvaccinated.
It can be said for certain age groups, certainly. But not all. We get e.g. Anaphylaxis as often as 5/1,000,000 from the vaccine (CDC). We don't get that many COVID-19 hospitalizations in e.g. the 0-15 age group, IIRC.
-
@lolwhat said in Tales from Coronavee-rooss Italy, mamma mia!:
@boomzilla said in Tales from Coronavee-rooss Italy, mamma mia!:
they went crazy about the vaccines and freaked people out even more
Even worse, here in the States, the protocol was - perhaps, still is - the following:
- "go back home and stay there until you have trouble breathing," by which time your blood O2 is not much above danger zone, if you're lucky - oh, and of course, no significant medication or other treatment is given when you present initially
- when you finally do go in, the hospital puts you on a vent, which is by itself known to be very difficult not to stop needing (except when you die, of course)
- the hospital also puts you on remdesivir, which is by itself known to cause potentially severe organ damage
Of course, in the world of corporate medicine, no one deviates from the protocol without a fight. Also, no one asks how many of the "COVID" deaths involved a vent, remdesivir, or being told to stay home until you have trouble breathing.
Same here. Do nothing, wait, admit to hospital, still do nothing, check if died.
@dkf said in Tales from Coronavee-rooss Italy, mamma mia!:
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
How would vaccinating fewer people lead to "less pressure on the virus to start evading vaccines that way"?
Ugh, evolution doesn't work that way. The formation of new variants is a random process — every time the virus reproduces you roll the dice to see if you get a new variant, and occasionally those new variants are better adapted to their environment — but if we can reduce the rate at which the virus reproduces then we increase the expected time to the appearance of new variants that are better able to avoid vaccine-induced immunity. The lower the overall population infection rate, the less likely you are to roll snake eyes somewhere and have a new pile of shit to deal with.
Uh, no. By mass vaccinating with a vaccine that doesn't massively reduce infection rate you create an environment which selects for vaccine resistance.
You have same probability of all possible mutations occuring in vaccinated and unvaccinated populations, but in vaccinated population vaccine resistance gives significant reproduction advantage.
-
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
@boomzilla said in Tales from Coronavee-rooss Italy, mamma mia!:
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
@boomzilla said in Tales from Coronavee-rooss Italy, mamma mia!:
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
@Gąska said in Tales from Coronavee-rooss Italy, mamma mia!:
@dkf the problem with hypothetical avoidable deaths is that there are infinitely many of them,
With a finite number of people alive?
and you cannot even estimate them most of the time. For example, if we didn't fast-track the vaccines, less people would be skeptical of them - and by today we'd end up with many more vaccinated.
No. By today we'd have precisely zero vaccinated outsides clinical trials, because the approval would be expected around 2025.
Most of the time savings in the fast-track process (aside from simply treating it as prio 1 in the bureaucracy of course) was from interleaving the trial phases, which is usually not done because you don't want to expose a large number of volunteers to something you haven't checked is safe. That interleaving has zero influence on the validity of the results.
Except we'd could have had more data on the medium term effects, i.e., the waning efficacy.
What could possibly have been the consequence of having this data?
a) go ahead and use the vaccine anyway
b) decide it's no good, wait without any vaccinations until we have developed something better and let it go through the multi-year approval process againAny other possibilities?
Edit:
by Also there could have been more focus on therapeutics. Aside from a governor or two here, it's been all about the vaccines.
What do you mean by "focus"? Do you see a lack of government funding for therapeutic research or would you just want politicians to talk about it more?
Sorry, in other posts I think that I was clearer about saying that I was talking about the messaging from public health officials (and people in the media, for that matter). That's what I was talking about, and the fact that there has been so much funding on therapeutics but such little communication is horrible.
In fact, one governor was attacked in the press for being very proactive about monoclonal antibodies. He set up multiple centers around his state for administering the antibodies (which had to be intravenously, so not as simple as giving people a pill) and a public campaign to make people aware of them and to encourage them to take advantage of the sites. Though to be fair, he was also attacked for being proactive about making vaccines easily available for residents (and also for some reason attacked as being anti-vaccine), but it goes to show how political the public communication has been as opposed to focused on relaying accurate medical information.
This is probably a bigger problem in the US than in most other places.
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
We don't get that many COVID-19 hospitalizations in e.g. the 0-15 age group, IIRC.
The main reason for wanting that age group to have a low infection rate is because they're a major route for spreading (all kinds of) infections around (to each other, to their families, to their teachers and other school staff). You might be able to get teens to mask up properly instead, but you will have all sorts of problems with kindergarteners.
-
@dkf New variants are not avoidable, as long as the disease's spread does not stop. You get the snake eyes eventually. The question is what happens after that.
To even attempt to do anything that takes advantage of the lower infection rate, you'd fist need to be certain that your vaccine does lower the infection rate in a meaningful way. Which it wasn't, before the current strategy was committed to. And then came the Delta and Omicron, so snake eyes were rolled first anyway.
-
@dkf said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
We don't get that many COVID-19 hospitalizations in e.g. the 0-15 age group, IIRC.
The main reason for wanting that age group to have a low infection rate is because they're a major route for spreading (all kinds of) infections around (to each other, to their families, to their teachers and other school staff). You might be able to get teens to mask up properly instead, but you will have all sorts of problems with kindergarteners.
So, vaccinate teens to slow the evolution. But never to stop it, mutations being an inescapable eventuality. All the while causing the side-effects on the <19 part of the population.
To sell that, you'd have to be able to show a very significant reduction in infection rate. Because I'm loathe to sell children's health for assumptions and wishes.
-
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
@boomzilla said in Tales from Coronavee-rooss Italy, mamma mia!:
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
@Gąska said in Tales from Coronavee-rooss Italy, mamma mia!:
@dkf the problem with hypothetical avoidable deaths is that there are infinitely many of them,
With a finite number of people alive?
and you cannot even estimate them most of the time. For example, if we didn't fast-track the vaccines, less people would be skeptical of them - and by today we'd end up with many more vaccinated.
No. By today we'd have precisely zero vaccinated outsides clinical trials, because the approval would be expected around 2025.
Most of the time savings in the fast-track process (aside from simply treating it as prio 1 in the bureaucracy of course) was from interleaving the trial phases, which is usually not done because you don't want to expose a large number of volunteers to something you haven't checked is safe. That interleaving has zero influence on the validity of the results.
Except we'd could have had more data on the medium term effects, i.e., the waning efficacy.
What could possibly have been the consequence of having this data?
a) go ahead and use the vaccine anyway
b) decide it's no good, wait without any vaccinations until we have developed something better and let it go through the multi-year approval process againAny other possibilities?
Edit:
by c) Mandate that people use the vaccine despite the potential risks and potential lack of benefit, which is the actual situation that a lot of people are finding themselves in.
-
@acrow And now I'm wondering if the mutation rate was ever controllable in the first place. After all, COVID spreads in multiple kinds of wildlife. Not all of them known to us.
For all we know, there might be more animal than human carriers already.
-
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
@boomzilla said in Tales from Coronavee-rooss Italy, mamma mia!:
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
@boomzilla said in Tales from Coronavee-rooss Italy, mamma mia!:
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
@Gąska said in Tales from Coronavee-rooss Italy, mamma mia!:
@dkf the problem with hypothetical avoidable deaths is that there are infinitely many of them,
With a finite number of people alive?
and you cannot even estimate them most of the time. For example, if we didn't fast-track the vaccines, less people would be skeptical of them - and by today we'd end up with many more vaccinated.
No. By today we'd have precisely zero vaccinated outsides clinical trials, because the approval would be expected around 2025.
Most of the time savings in the fast-track process (aside from simply treating it as prio 1 in the bureaucracy of course) was from interleaving the trial phases, which is usually not done because you don't want to expose a large number of volunteers to something you haven't checked is safe. That interleaving has zero influence on the validity of the results.
Except we'd could have had more data on the medium term effects, i.e., the waning efficacy.
What could possibly have been the consequence of having this data?
a) go ahead and use the vaccine anyway
b) decide it's no good, wait without any vaccinations until we have developed something better and let it go through the multi-year approval process againAny other possibilities?
Edit:
by Also there could have been more focus on therapeutics. Aside from a governor or two here, it's been all about the vaccines.
What do you mean by "focus"? Do you see a lack of government funding for therapeutic research or would you just want politicians to talk about it more?
To expand on @boomzilla's point, the existence of effective therapeutics doesn't necessarily undercut the rationale for vaccines. But it undercuts the rationale for vaccine mandates.
Here in the US, the choice is presented, politically and in the media, as binary between "get the vaccine" or "die of COVID."
When in fact, the vaccines are more dangerous and less effective than they were portrayed. And the existence of effective therapeutics undercuts the rationale further.
-
@dkf said in Tales from Coronavee-rooss Italy, mamma mia!:
You might be able to get teens to mask up properly instead
Please define properly.
-
@lolwhat said in Tales from Coronavee-rooss Italy, mamma mia!:
@dkf said in Tales from Coronavee-rooss Italy, mamma mia!:
You might be able to get teens to mask up properly instead
Please define properly.
Let us maybe not go there again. I think we can all agree that masking the general populace was not a shining success story. Whether teens were properly masked is moot, if even their elders find it hard.
-
@acrow Hell, trained medical personnel in hospitals were not properly masked for the longest time, depending on which mask efficiency studies we read. And still are not masked to the standard I'd prefer (closed-circuit rebreathers). Or even increased the goddamn ventilation, even though it'd make more difference than either of the aforementioned.
So can we all please forgo the masks and the teens for today?
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
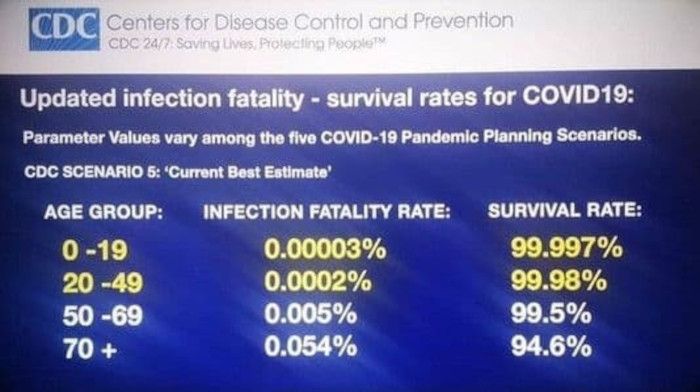
Can someone help me make sense of that table? Are the two sides sipposed to add up to 100%? Did they make a mistake and one of the columns is off by a factor of 100? If not, then what's the difference between the two metrics and how come there's exactly 100x difference all four times?
-
@Gąska said in Tales from Coronavee-rooss Italy, mamma mia!:
Did they make a mistake and one of the columns is off by a factor of 100?
I'd guess that the central column just had a "%" mark put on the end of it instead of being handled properly. It's the sort of fuck up that happens when making a presentation quickly.
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
What's the numeric risk of not surviving the vaccine for the 0-19 group?
Death is not the only issue. Some of the other side-effects are rather bad too. E.g.:
Obviously. We can compare the frequency of those when we include other non-lethal effects of infections, too. But as you cited infection fatality ratios only, let's compare equal risks, shall we?
Why would you believe your infection fatality rates from the same source are based on solid evidence if the infection rates they are based on are not?
Because the count of deaths has a known source material (death certificates) available to the reporting entity (U.S. CDC), which reports all of them. And it's plausible that they can find out the vaccination status of each dead person. So it's technically plausible to count this number, even though the died from vs died with debate puts its exactness to some doubt.
Whereas infections are based on people's reporting only. There's no population screening, or any mechanism that would give a rate without human bias. And people who got the vaccination are biased to believe that their couch is not COVID, since they are vaccinated.
It's called an "infection fatality ratio" because it gives the ratio of infections to deaths. To know the infection status of all the deceased is obviously not enough to calculate that. You need a good estimate for the total number of infections. Which you say the CDC doesn't have.
You said there is "no evidence" that "vaccines limit infection". How would vaccinating fewer people lead to "less pressure on the virus to start evading vaccines that way"?
"No evidence" does not mean that it can't happen. It just means we can't know whether it happens or not. And if it limited infection, then it soon won't, so the point is moot.
 OK, @dkf tried to explain that point already, I don't have anything to add.
OK, @dkf tried to explain that point already, I don't have anything to add.
-
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
It's called an "infection fatality ratio" because it gives the ratio of infections to deaths. To know the infection status of all the deceased is obviously not enough to calculate that. You need a good estimate for the total number of infections. Which you say the CDC doesn't have.
This is where having a more global perspective helps, as it lets you get a better estimate of the ratio of hospitalizations to infections using the fact that some countries have stronger population-level monitoring than the CDC does. (This is under the assumption that the biology of the disease is fundamentally similar in different countries, which I believe is the case within a variant. The various variants are known to be different from each other in behaviour.) Hospitalizations and deaths are both nice observables as there's mostly a global agreement on the meaning of them (not 100% match, but close), though they are both lagging and noisy indicators (especially the death data, which is very very noisy in raw form).
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@dkf said in Tales from Coronavee-rooss Italy, mamma mia!:
One thing that can be said is that the rate of serious side effects from the majority of vaccines in deployment appear to be multiple orders of magnitude lower than the population average rate of serious outcomes from coronaviral infections among the unvaccinated.
It can be said for certain age groups, certainly. But not all. We get e.g. Anaphylaxis as often as 5/1,000,000 from the vaccine (CDC). We don't get that many COVID-19 hospitalizations in e.g. the 0-15 age group, IIRC.
5696 in the 0-17 age group since April 2020. That age cohort is about 74M people, so you'd expect about 370 cases of anaphylaxis. 15 times fewer.
-
@dkf said in Tales from Coronavee-rooss Italy, mamma mia!:
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
It's called an "infection fatality ratio" because it gives the ratio of infections to deaths. To know the infection status of all the deceased is obviously not enough to calculate that. You need a good estimate for the total number of infections. Which you say the CDC doesn't have.
This is where having a more global perspective helps, as it lets you get a better estimate of the ratio of hospitalizations to infections using the fact that some countries have stronger population-level monitoring than the CDC does. (This is under the assumption that the biology of the disease is fundamentally similar in different countries, which I believe is the case within a variant. The various variants are known to be different from each other in behaviour.) Hospitalizations and deaths are both nice observables as there's mostly a global agreement on the meaning of them (not 100% match, but close), though they are both lagging and noisy indicators (especially the death data, which is very very noisy in raw form).
Yeah, I'd think Finland would probably have this data if @acrow cared to look. As for me,

-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
the more severe the fatality
I don't think fatality really has degrees of severity (unless you believe in some sort of post-death reward/punishment, but that's not what we're talking about in this thread). Different causes of fatality have different degrees of suffering preceding fatality, but fatality itself is fatal.
-
@HardwareGeek what about the little death?
-
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@dkf said in Tales from Coronavee-rooss Italy, mamma mia!:
One thing that can be said is that the rate of serious side effects from the majority of vaccines in deployment appear to be multiple orders of magnitude lower than the population average rate of serious outcomes from coronaviral infections among the unvaccinated.
It can be said for certain age groups, certainly. But not all. We get e.g. Anaphylaxis as often as 5/1,000,000 from the vaccine (CDC). We don't get that many COVID-19 hospitalizations in e.g. the 0-15 age group, IIRC.
5696 in the 0-17 age group since April 2020. That age cohort is about 74M people, so you'd expect about 370 cases of anaphylaxis. 15 times fewer.
So we get 370 extra cases of Anaphylaxis in young people this year just from the vaccines? Is that good or bad, in your opinion? Because it sounds kinda bad to me.
Then again, I'm a parent. So even a remote chance of anaphylaxis in my children's age group is bad to me.
-
@boomzilla said in Tales from Coronavee-rooss Italy, mamma mia!:
There's been a lot of noble lying on public health.
I'm not sure about the "noble" part. Yeah, most likely some people really do think the lies they're pushing are beneficial to the public, but I see a lot of them as self-serving and/or forcing social change the public would not otherwise accept.
-
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
@dkf said in Tales from Coronavee-rooss Italy, mamma mia!:
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
It's called an "infection fatality ratio" because it gives the ratio of infections to deaths. To know the infection status of all the deceased is obviously not enough to calculate that. You need a good estimate for the total number of infections. Which you say the CDC doesn't have.
This is where having a more global perspective helps, as it lets you get a better estimate of the ratio of hospitalizations to infections using the fact that some countries have stronger population-level monitoring than the CDC does. (This is under the assumption that the biology of the disease is fundamentally similar in different countries, which I believe is the case within a variant. The various variants are known to be different from each other in behaviour.) Hospitalizations and deaths are both nice observables as there's mostly a global agreement on the meaning of them (not 100% match, but close), though they are both lagging and noisy indicators (especially the death data, which is very very noisy in raw form).
Yeah, I'd think Finland would probably have this data if @acrow cared to look. As for me,
We don't have it either. The testing was too selective for most of the pandemic. And then people got tired of it.
To get that kind of data, you'd need either very, very eager testing from any sumptoms, or mass screenings. And the only country that did that level of screening, China, just broke the news that some of their labs have been returning false negatives while overwhelmed. So nobody has a really accurate count.
-
@HardwareGeek I meant fatality rate. Morbidity. What's the word again? Lethality?
Please excuse my Finnish while I'm concentrating on work.
-
@HardwareGeek said in Tales from Coronavee-rooss Italy, mamma mia!:
@boomzilla said in Tales from Coronavee-rooss Italy, mamma mia!:
There's been a lot of noble lying on public health.
I'm not sure about the "noble" part. Yeah, most likely some people really do think the lies they're pushing are beneficial to the public, but I see a lot of them as self-serving and/or forcing social change the public would not otherwise accept.
Well, they were lying because they think it's better for the public. That's the definition. I think it's pretty clear that their judgement was wrong, if only because they subsequently lost so much public credibility.
Then there's stuff like shutting down on the lab leak theory (and covering up their own complicity) and rationalizing that it's better for "international harmony" to deny it.
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@dkf said in Tales from Coronavee-rooss Italy, mamma mia!:
One thing that can be said is that the rate of serious side effects from the majority of vaccines in deployment appear to be multiple orders of magnitude lower than the population average rate of serious outcomes from coronaviral infections among the unvaccinated.
It can be said for certain age groups, certainly. But not all. We get e.g. Anaphylaxis as often as 5/1,000,000 from the vaccine (CDC). We don't get that many COVID-19 hospitalizations in e.g. the 0-15 age group, IIRC.
5696 in the 0-17 age group since April 2020. That age cohort is about 74M people, so you'd expect about 370 cases of anaphylaxis. 15 times fewer.
So we get 370 extra cases of Anaphylaxis in young people this year just from the vaccines? Is that good or bad, in your opinion? Because it sounds kinda bad to me.
Then again, I'm a parent. So even a remote chance of anaphylaxis in my children's age group is bad to me.
But the 5696 cases of covid hospitalizations are not?
-
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
Obviously. We can compare the frequency of those when we include other non-lethal effects of infections, too. But as you cited infection fatality ratios only, let's compare equal risks, shall we?
Fine. I've got numbers from Finland for 2020. Those good?
Deaths in the age group 0-19 while Sars-CoV2 -positive: 0.
Deaths in age group 20-24 for same: 1.I hear some diabetic teens died
this yearin 2021. But no statistics yet. The official page for the statistics agency says that the statistics for 2021 will not be published until end of 2022.
Edit: fixed year
-
@dkf said in Tales from Coronavee-rooss Italy, mamma mia!:
they're a major route for spreading (all kinds of) infections around (to each other, to their families, to their teachers and other school staff).
Kids are germ factories.
Increased human fertility is an evolutionary mechanism for microorganisms to increase their own rate of spread. Change my mind.
-
@topspin said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@dkf said in Tales from Coronavee-rooss Italy, mamma mia!:
One thing that can be said is that the rate of serious side effects from the majority of vaccines in deployment appear to be multiple orders of magnitude lower than the population average rate of serious outcomes from coronaviral infections among the unvaccinated.
It can be said for certain age groups, certainly. But not all. We get e.g. Anaphylaxis as often as 5/1,000,000 from the vaccine (CDC). We don't get that many COVID-19 hospitalizations in e.g. the 0-15 age group, IIRC.
5696 in the 0-17 age group since April 2020. That age cohort is about 74M people, so you'd expect about 370 cases of anaphylaxis. 15 times fewer.
So we get 370 extra cases of Anaphylaxis in young people this year just from the vaccines? Is that good or bad, in your opinion? Because it sounds kinda bad to me.
Then again, I'm a parent. So even a remote chance of anaphylaxis in my children's age group is bad to me.
But the 5696 cases of covid hospitalizations are not?
Oh. I thought he meant there were 5696 cases of anaphylaxis in the age group. Didn't bother opening the link. My bad.
Still, based on the observed effect on teens in Finland, that figure seems rather high to me. I have to ask whether these are hospitalizations from COVID, or with COVID. Because the U.S. officials recently admitted their statistics mixing the two.
Also, whether they were already seriously ill or not. It's not reasonable to group the healthy teens with those with serious pre-existing conditions like diabetes.
-
@topspin said in Tales from Coronavee-rooss Italy, mamma mia!:
it seems more likely that the effectiveness against infection actually just reduced in newer variants, maybe even that that original effectiveness was slightly lower than estimated, than that they ordered new variants to cover up their partial lie about one aspect of the study that the effectiveness was zero to begin with.
Listen I don't spend 2 hours a day waxing this mustache not to be Cartoon Evil.
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
@dkf said in Tales from Coronavee-rooss Italy, mamma mia!:
One thing that can be said is that the rate of serious side effects from the majority of vaccines in deployment appear to be multiple orders of magnitude lower than the population average rate of serious outcomes from coronaviral infections among the unvaccinated.
It can be said for certain age groups, certainly. But not all. We get e.g. Anaphylaxis as often as 5/1,000,000 from the vaccine (CDC). We don't get that many COVID-19 hospitalizations in e.g. the 0-15 age group, IIRC.
5696 in the 0-17 age group since April 2020. That age cohort is about 74M people, so you'd expect about 370 cases of anaphylaxis. 15 times fewer.
So we get 370 extra cases of Anaphylaxis in young people this year just from the vaccines? Is that good or bad, in your opinion? Because it sounds kinda bad to me.
In the context of the reduction in COVID hospitalizations, that's awesome, even disregarding that most of these reactions are resolved with an epi-pen and a night or two for observation if you're unlucky—hardly comparable to a hospital stay with COVID.
Then again, I'm a parent. So even a remote chance of anaphylaxis in my children's age group is bad to me.
Sometimes kids burn alive because they couldn't get out of their seatbelt quickly enough. Sounds kinda bad to me, too. I still tell my son to put on a seatbelt because statistics.
-
@LaoC Right. So those 5696. Were they previously healthy teens? And did they go to the hospital because of COVID, or did it get discovered afterwards?
-
@GuyWhoKilledBear said in Tales from Coronavee-rooss Italy, mamma mia!:
the vaccines are more dangerous and less effective than they were portrayed.
Especially the "less effective" part. Vaccines have been portrayed as a panacea. If everybody is vaccinated, COVID will just stop. Nobody will die; nobody will even get sick. However, that has never been the truth of the vaccines; they were never intended to prevent infection. The clinical testing wasn't even designed to measure that. But that's how vaccination has been pushed on the public.
And the public propaganda doesn't even mention side effects.
-
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
I have to ask whether these are hospitalizations from COVID, or with COVID.
It's funny that this always gets mentioned for Covid cases, but then we're talking about VAERS data which doesn't even claim to make this distinction, as anybody can report anything that happened post hoc, so is massively overreported with background signal.
-
@LaoC said in Tales from Coronavee-rooss Italy, mamma mia!:
Sometimes kids burn alive because they couldn't get out of their seatbelt quickly enough.
Do they? Can't find any source. And I'm not just being contrarian; it seems like one of those things that everyone assumes must necessarily happen from time to time because it sounds logical, but there seem to be no actual examples of it.
-
-
@topspin said in Tales from Coronavee-rooss Italy, mamma mia!:
@acrow said in Tales from Coronavee-rooss Italy, mamma mia!:
I have to ask whether these are hospitalizations from COVID, or with COVID.
It's funny that this always gets mentioned for Covid cases, but then we're talking about VAERS data which doesn't even claim to make this distinction, as anybody can report anything that happened post hoc, so is massively overreported with background signal.
Actually, only medical personnel can report to VAERS. So over-counting is unlikely.
And I assume that the report contents are more useful than what we have in Finland.